 Chris N. W. Geraets
Chris N. W. Geraets Märta Wallinius1,2,4
Märta Wallinius1,2,4 Kristina Sygel
Kristina Sygel- 1Lund Clinical Research on Externalizing and Developmental Psychopathology, Child and Adolescent Psychiatry, Department of Clinical Sciences Lund, Lund University, Lund, Sweden
- 2Research and Development Unit, Regional Forensic Psychiatric Clinic, Växjö, Sweden
- 3Department of Psychiatry, University Medical Center Groningen, Groningen, Netherlands
- 4Department of Psychiatry and Neurochemistry, Centre for Ethics, Law and Mental Health, Institute of Neuroscience and Physiology, The Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden
- 5Department of Forensic Psychiatry, National Board of Forensic Medicine, Stockholm, Sweden
Background: Technological developments such as Virtual reality (VR) provide new opportunities to extend and innovate mental healthcare. VR as a tool for clinical assessment has been described as promising, as it can enable real-time assessment within real-like environments or contexts as opposed to self-report and behavioral tasks in laboratory settings.
Objective: With this systematic review we aimed to provide an overview of recent studies using VR in the assessment of psychiatric disorders.
Methods: A systematic search was performed using Pubmed, Embase, PsycInfo, and Web of Science between 2016 and 2020. Studies were included if they used immersive VR, concerned assessment of psychiatric symptoms/disorders, and included adult patients with psychiatric disorders.
Results: The search resulted in 3,163 potentially eligible articles, from which a total of 27 studies fulfilled inclusion criteria. Most studies considered anxiety (n = 7), addictive, (n = 7), or psychotic disorders (n = 5). Regarding ADHD (n = 3), PTSD (n = 3), and pedophilic disorder (n = 1), a few studies had been performed since 2016. The majority of the included studies compared patient groups to healthy control groups.
Discussion: Recent studies on VR-assisted psychiatric assessments have been conducted to validate VR environments, to assess symptoms for diagnostics or therapy goals, search for biomarkers, and to gain knowledge on psychiatric disorders. VR tasks were able to detect some difference between patient and healthy control groups, mainly with regard to self-report measures. Despite previous, promising prospects, the use of VR as a tool in clinical assessments must still be considered as a field in need of continued developments and evaluations.
Systematic Review Registration: www.crd.york.ac.uk/prospero, identifier: CRD42021233772.
Introduction
Assessments and the diagnostic process in psychiatry mainly consist of clinical interviews, self-report questionnaires, neuropsychological tests, and, in some cases, behavioral observations (1). Such assessments constitute a basis for the individual tailoring of psychiatric treatment for patients. However, interviews and self-report questionnaires strongly rely on patients' memory, current mental state, self-understanding, and insight. Also, the context within which psychiatric assessments are performed may be criticized for lack of ecological validity. Therefore, a need for ecologically valid psychiatric assessments with increasingly objective measures has been expressed, and method developments thereto related are needed (2).
Novel technologies, such as immersive virtual reality (VR), may provide new possibilities in the quest to fill this gap (3, 4). With immersive VR, patients enter computer-generated simulations, e.g., going to a grocery store, by using a head-mounted display or CAVE environment. Such immersive systems can deliver a fully surrounding, extensive and vivid illusion of reality to people's senses (5). VR simulations have been shown to trigger psychological and physical reactions similar to the reactions in real life (6). This feature—feeling real—makes VR a promising tool for psychiatric assessments (7). This perceived realness of a VR experience or the feeling of being “there” is called presence (8). Presence is the subjective illusion of being in a real place despite being physically located in a different place, causing people to react realistically to the VR (9). Furthermore, VR has the advantage that you can (repeatedly) expose patients to (social) situations that are completely controlled and can be accessed within a safe, clinical environment. Thus, the same VR social environment can be presented to multiple patients to assess, cognitions, behaviors, emotions, and physiological responses in real-time. Given this, VR-assisted psychiatric assessment has been described as promising as it may enable real-time assessments within (individually tailored) virtual environments or contexts that are perceived and experienced by the patient as “real.” This can create greater possibilities for increased ecological validity of psychiatric assessments as opposed to assessments relying on self-reports, interviews, and behavioral tasks conducted in laboratory settings (10, 11).
To date, two systematic reviews have investigated the existing evidence on VR-assisted psychiatric assessments up to 2016 (10, 12). van Bennekom et al. (12) identified 39 studies, mostly focusing on patients with a psychotic (n = 15) or developmental disorder (n = 12). The most common topics were paranoia and social behaviors. The authors concluded that almost all reviewed VR situations/scenarios enabled eliciting and measuring psychiatric symptoms to some extent. E.g., paranoid ideation has been measured in patients with psychotic disorders by exposing them to neutral VR environments (13, 14). The benefit of applying VR in such assessments lies in the fact that with self-report it is unknown whether reported hostility as experienced by the patient is real or not (15). In a controlled, VR environment with only neutral cues, a patient's self-reported level of perceived hostility in the VR environment then becomes easier to evaluate objectively. Supporting the validity of VR-assisted psychiatric assessments, van Bennekom et al. (12) found significant relations between VR measures and traditional diagnostic measures in 14 studies. However, relatively small groups were tested, limiting definite conclusions.
Similarly, Freeman et al. (10) concluded, in a broader systematic review on 285 studies (of which 86 considered assessments), that psychiatric symptoms can be assessed with VR, but that this at the time of the systematic review predominantly had been done to validate VR environments or gain an increased understanding of symptoms and mechanisms of psychiatric disorders, rather than for clinical assessment purposes. Also, the evidence for reliability and validity (e.g., convergent validity in relation to common self-report measures) for VR-assisted psychiatric assessments was demonstrated as very limited.
Over the past years, research on VR applications for mental healthcare has been rapidly expanding due to decreased costs and improved quality of software and hardware, and an update of the evidence-base for VR-assisted psychiatric assessments is needed. Therefore, this study aimed to provide a systematic review of recent studies (from 2016 onwards) applying immersive VR in psychiatric assessments. To this end, we reviewed VR assessment studies on differences between patients with a psychiatric disorder and healthy controls, and studies investigating the relation between VR measures and established diagnostic measures e.g., clinical assessments or patient-rated questionnaires of psychiatric symptoms and disorders.
Methods
Design
We conducted a systematic review on trials applying immersive VR in the assessment of psychiatric symptoms and disorders. This review was registered on PROSPERO (CRD42021233772). Two previous systematic reviews have described, in detail, the studies conducted up to 2016 (10, 12). This systematic review focuses on more recent findings reported between 01-01-2016 and 31-12-2020.
Inclusion and Exclusion Criteria
Inclusion criteria were: (1) use of immersive VR (utilizing a head-mounted-display (HMD) or CAVE), (2) concerning assessment of psychiatric symptoms or disorders, (3) either comparing a patient group with a healthy control group or investigating the relation between a VR and an established measure, (4) concerning adult patients with a psychiatric disorder, (5) original empirical research findings (e.g., pilot, RCT, or case-series), (6) published in an English peer-reviewed journal, and (7) published between 01-01-2016 and 31-12-2020.
Exclusion criteria were: (1) letters to editors, theses, conference papers, or book chapters, (2) participants with primarily learning and intellectual disabilities, (3) full text unavailable, (4) unclarities concerning which VR technology was applied, and (5) one-to-one VR computerized version of a neuropsychological test.
Literature Search and Study Selection
Four databases were searched: PubMed, PsychInfo, Web of Science, and Embase. See Supplementary Material 1 for the complete search strategies. For each of the following diagnostic/patient groups, specific search terms were created and added to the search: anxiety disorders, mood disorders, psychotic disorders, eating disorders, autism, ADHD, substance use disorders, impulse control disorders, sexual disorders, personality disorders, forensic psychiatry, and mental health generally. Databases were searched from 01-01-2016 up until 31-12-2020. The general keyword search terms were: Virtual reality OR “VR technology” AND assess* OR diagnos* OR test OR experiment OR evaluation AND—specific terms for each patient group.
First, duplicate references were removed and titles and abstracts were read to screen for relevant studies. Then, two researchers independently reviewed the full texts to determine whether the inclusion and exclusion criteria were met. Consensus between the researchers (CG and KS) was a prerequisite for inclusion, differences in judgment were solved by discussion between the two researchers.
Quality Assessment
The Quality Assessment Tool for Quantitative Studies (QATQ) of the Evaluation of Public Health Practise Project was used for quality assessments of the included studies (16). Studies were rated on six domains: selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs. The QATQ provided a global rating based on the subscales: strong = no weak ratings, moderate = one weak rating, or weak = two or more weak ratings on the subscales.
Results
The final search was conducted on 23-02-2021 and, after duplicate removal, this resulted in 3,163 identified articles. In total, 27 articles met the inclusion criteria, see Figure 1 for a flowchart of the search. Two of the 27 studies concerned a follow-up publication to an original study (17, 18) that was also included. In total, these studies included 2,121 participants, of whom 1,123 were patients with psychiatric disorders and 998 were healthy controls. The most common reasons for studies not to be included during the full-text screening procedure were the use of non-immersive VR (e.g., use of 2d computer screens/desktops) and lack of a psychiatric patient group in the study.
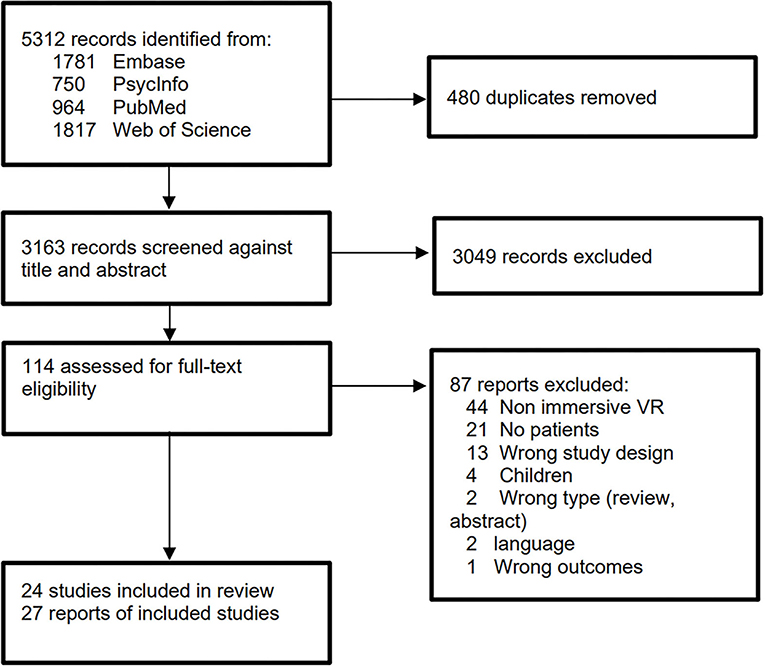
Figure 1. Flow diagram of the study inclusion process.
Table 1 provides a summary of the included studies, presented per diagnostic subcategory. Most studies were performed on assessment of anxiety (n = 7), addictive (n = 7), or psychotic disorders (n = 5). Concerning, ADHD (n = 3), PTSD (n = 3), and pedophilic disorder (n = 1), only a few studies have been performed since 2016. Table 2 presents an overview of the results of the quality assessment for each study. Ten studies were of moderate quality, and 17 demonstrated a strong quality rating.
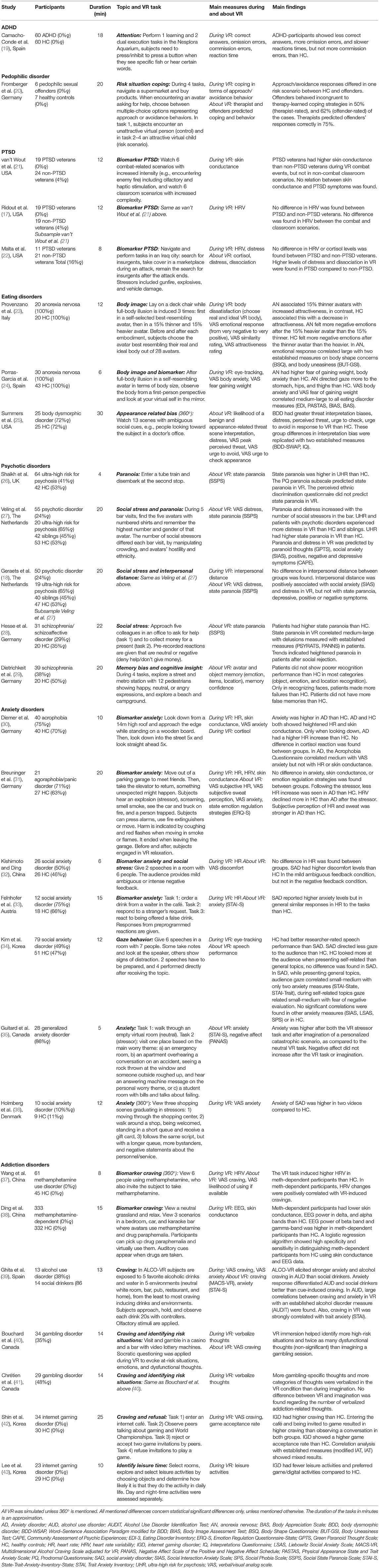
Table 1. VR-assisted psychiatric assessments.
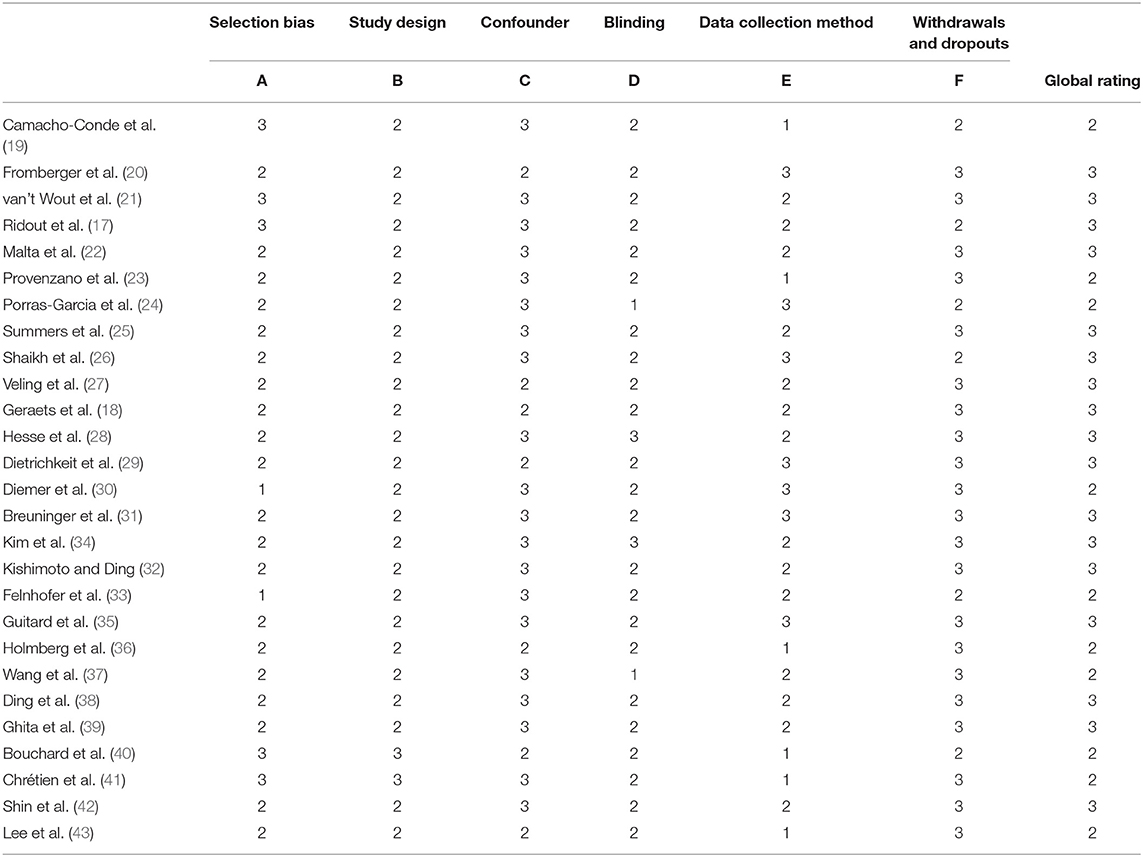
Table 2. Immersive VR-assisted psychiatric assessment studies EPHPP quality rating.
Discussion
With this systematic review, we aimed to provide an overview of recent (2016–2020) publications on immersive VR-assisted psychiatric assessment. In total, 27 studies were identified, however, the goals of assessment differed significantly, ranging from assessment of symptoms for diagnostics, to give direction to therapy, search for biomarkers, or to be used in research for gaining increased understanding of a disorder. First, the findings per diagnostic group will be discussed.
Recent VR-Assisted Psychiatric Assessment Studies
Developmental Disorders
Research on VR assessment in adults with developmental disorders was very limited. A single study on ADHD was identified, comparing young, mostly adult, males with and without ADHD (19). Similar to research in children, this study concerned a VR-assisted neuropsychological test (Nesplora Aquarium test) that continues the wave of 2D computerized continuous performance tasks for assessment of attention, working memory, and processing speed (12). No studies were identified on autism spectrum disorders (ASD). The objective of using new technologies for assessment is often to make a diagnosis as early as possible. As ASD is a developmental disorder this may explain the lack of research in adults. However, recent reviews including children with ASD show a similar gap in knowledge on the utility of VR for assessment (44, 45).
Pedophilic Disorder
One feasibility study has been conducted in the field of forensic psychiatry since the first research by Renaud et al. in offenders with a pedophilic disorder (46, 47). In this study, Fromberger and colleagues tested, in pedophilic sex offenders, whether coping behaviors in VR risk scenarios—encountering children asking for help in a supermarket—can provide additional information for risk assessments (20). Many offenders behaved differently in VR than their own beliefs about desired responses and coping strategies they had focused on in treatment. Also, therapists predicted offender's behavior wrongly 25% of the time. This indicates that VR-assisted assessments can add a new dimension to risk assessments by testing, in a safe environment, whether learned or desired strategies transfer to behavior. Especially in forensic settings, this can be useful as behavior assessments on risk situations in real life would be highly unethical. Furthermore, applying VR-assisted risk assessments could in part counteract the social desirability which is common among offenders self-reporting on their own intended behaviors related to offending. However, the authors indicated that further development of the task was needed, in terms of response possibilities and the creation of scenarios with fewer moral dilemmas.
PTSD
VR-assisted assessment in PTSD has mainly focused on differentiating between veterans with and without PTSD by using physiological measures during VR exposure to combat situations (17, 21, 22). However, only differences in skin conductance level (21), but not in heart rate variability (HRV) (17, 22) nor cortisol levels (22), were found between groups. The difference in skin conductance was specific for combat situations, in a classroom environment no such difference was found. Interestingly, the skin conductance (21) and HRV (17) research concerned the same sample, suggesting that skin conductance measures may be more sensitive. Similarly, van Bennekom et al. also identified one study in PTSD, also showing heightened skin conductance in PTSD veterans compared to healthy controls (48).
Eating Disorders
Whereas, previous assessment research in eating disorders has mainly focused on the reaction of patients to virtual food (12), three recent studies have focused on body image and appearance-related biases. Two studies on anorexia nervosa used the technique of body illusion or embodiment (23, 24). Embodiment refers to the illusion that a virtual life-sized body, seen from a first-person perspective, is experienced as one's own body (49, 50). Medium to large correlations were found between established self-report questionnaires on eating disorders and single item VR VAS measures on fear of gaining weight, body anxiety, and emotional responses (23, 24). Further, anorexia patients felt more negative emotions after being embodied in a heavier body than a thinner one than their own. Healthy controls showed opposite reactions; feeling more negative in thinner bodies than heavier ones (23). Furthermore, clear distinctions between controls and patients were found with eye-tracking; anorexia patients directed their gaze to different parts of the body than healthy people (24). Summers et al. used VR differently, showing ambivalent 360° videos (e.g., overhearing a conversation about someone else's appearance) to patients with a body dysmorphic disorder and focused on interpretation bias (25). Also here, differences to controls were found in interpretation and emotional reactions to the VR scenes, consistent with well-established measures. The authors concluded that VR assessment may help to provide more nuanced treatment targets.
Psychotic Disorders
Following previous work on psychosis (10, 12), recent VR-assisted assessments have been done to measure paranoia, social stress, and memory bias in patients with a psychotic disorder or at ultra-high risk for psychosis. Consistently paranoid thoughts, measured by the State Social Paranoia Scale (51) were triggered in patients (18, 26–28, 51). Important to note, the VR paranoia tasks of these studies differed in content; Shaikh and colleagues exposed people to a neutral tube train ride (26), whereas the other studies exposed people to situations differing in the amount of social stress (e.g., being in a bar with neutral or hostile looking people (18, 27), or asking help from colleagues and receiving neutral or negative reactions (28).
Anxiety Disorders
In the domain of anxiety, VR has mainly been used to investigate feelings of anxiety and physiological responses during general stressful and social interaction situations (e.g., where participants had to give a speech or respond to a stranger in a bar). All studies reported that patients with an anxiety disorder consistently showed higher levels of subjectively experienced anxiety, except for Breuninger et al. who found that similar levels of anxiety were provoked during a VR emergency situation (fire in a parking garage). Concerning physiological measures, skin conductance (30, 31), cortisol (31), heart rate (30–33), and eye-tracking (34) were measured. No differences in skin conductance, nor cortisol reactions, were found between patients and controls. Regarding heart rate measures, reactions in VR environments tended to be similar in controls and patients (30, 32, 33), with two studies showing some differences when zooming in on specific stressor moments (30, 33). Interestingly, Breuninger et al. showed that the subjective perception of sweat and heart rate differed strongly between patients and controls, in contrast to the actual physiological measures. These findings contrast to the Bennekom et al. review (12), which concluded that most physiological measures were in accordance with subjective anxiety measures.
Addictive Disorders
Seven articles were found on addictive disorders, ranging from methamphetamine and alcohol disorders to gambling and gaming disorders, mainly studying craving. Many different types of designs were used, with 5/7 studies having a control group, and some measuring only biological markers. Differences between patients and controls were found in both craving and anxiety in alcohol disorder (39) and internet gaming disorder (42), as well as differences in physiological reactions for methamphetamine disorder (HRV and EEG) (37, 38). Two studies used VR in the context of treatment (40, 41). Engaging in virtual gambling was used in both studies in combination with Socratic questioning to identify risk situations, where participants had to verbalize their thoughts during the VR exposure. The researchers found that patients reported more dysfunctional thoughts and more categories of thoughts during VR exposure than during mental imagery. Based on this, the visual component of VR may be helpful to identify risk situations and treatment targets for patients with addictive disorders.
VR Task Characteristics
Task characteristics differed substantially on several factors, such as the type of VR used, level of social and object interaction, level of personalization, and modalities used e.g., smell and touch. No ideal task characteristics seem to be identifiable, as e.g., the amount of interaction and personalization needed seems to vary strongly with the specific goal and purpose of the assessment. Three studies used 360° videos to assess anxiety, craving, and interpretation bias in body dysmorphic disorder. Although 360° videos limit interaction and personalization, they do offer standardized, easy, and cheap applications. In four of the 27 studies, some form of personalization was applied to the VR program. In two studies, self-resembling avatars were made for body image assessment (23, 24). Further, in the research of Fromberger et al., virtual child characters were selected before the assessment based on the sexual offender's level of attraction to them (20). Guitard et al. (35) personalized the task based on the main worry theme of a person. Three anxiety-inducing situations were available to choose from which fitted the worry theme best (an emergency room, apartment, or a student room scenario), and in one of them, people would hear a message on an answering machine based on their personal worry theme.
The Future of VR-Assisted Psychiatric Assessments
In line with the earlier reviews, all VR tasks were able to detect some difference between patient groups with a psychiatric disorder and healthy control groups, with regard to self-report measures (10, 12). However, the road from research to clinical practice, to apply VR for diagnostic purposes and provide direction for psychiatric treatment, seems still substantial. Most of the tasks applied so far are lacking reliability and validity, and no test-retest designs were identified. In general, samples were small, with 60% including patient groups of maximally 30 people. Further, concerning behavioral tasks, a comparison between VR and real-world behavior is lacking. In order to answer the question as to how VR can affect the ecological validity of psychiatric assessments, such studies are needed.
Concerning physiological measures, findings were less convincing than studies including self-report measures. In several studies, similar responses were observed in patients and controls. E.g., veterans with PTSD did not differ in HRV or cortisol from veterans without PTSD during VR combat scenarios, findings on heart rate in anxiety-inducing situations were mixed, and interpersonal distance regulation in response to social stressors did not differ between people with different psychosis liability. These findings pose questions about the usefulness of physiological measures for psychiatric assessment, despite their potential as an “objective” measure. When physiological measures are used during VR, this is done to measure real-time reactions in response to scenarios or specific stimuli. During VR, people often move, see multiple things which contrast strongly to controlled laboratory settings in which physiological measures are usually performed, which may induce error in the instrument readings. Possibly baseline measures—and not reactive measures to complex stimuli such as VR– may be more valuable in psychiatric assessments.
An important conclusion that may be drawn from the current study is that a knowledge gap still exists on the value and possible benefits of VR-assisted assessments as an addition to current psychiatric diagnostic processes. In coming research, it would be relevant to study what additional information VR-assisted assessments can provide next to other assessments, instead of evaluating VR as a substitute to more conventional psychiatric assessments. Fromberger et al. made a first step in this with research on pedophilic offenders (20). Furthermore, in clinical practice, assessments can also be intertwined with treatment. For example, during a VR-based CBT intervention, safety behaviors were continuously observed and paranoid thoughts were explored and emphasized on (52). Similarly, Riches et al. assessed paranoid ideation with interviews after VR exposure in a non-clinical high trait paranoia group, and concluded that themes identified through this assessment could help inform target areas for treatment (53). This form of assessment was also explored by the research group of Bouchard (40, 41), who analyzed verbalized thoughts of patients prompted by Socratic questioning during VR exposure to gambling situations. Thus, the potential of VR in combined assessment and treatment should be further investigated.
One other objective pursued by applying new technologies such as VR for assessment is to find alternative ways of classifying patients. This has been specifically addressed in frameworks investigating mental disorders, such as the Research Domain Criteria (RDoC), where it is argued that the understanding of mental disorders through observable behaviors and self-reports should be complemented by other, so-called, units of analysis that are objectively collected e.g., with (neuro)physiological measures (54). This may allow obtaining new patient stratifications that better explain their response to treatment. Thus, for future research it is not only of relevance to investigate the relationship between a VR and an established measures but also to provide new measures (biomarkers) that could better explain the different phenotypes related to mental health.
Future research may also take advantage of qualitative approaches, e.g., with a more hypothesis-generating character. VR tasks can trigger feelings and cognitions which can be discussed during or after the VR task. Such an approach may be less objective but could turn out to be highly relevant in clinical practice. Also, other (neuro)physiological measures such as pupil dilation and saccadic eye movements, previously suggested as biomarkers for mental disorders, should be investigated using VR eye-tracking technology, in line with suggestions by the RDoC framework (55, 56). Future research should also further investigate the so-called Proteus effect (57). This effect shows that when using embodiment, characteristics of the embodied avatar can also influence an individual. E.g., people embodied in taller avatars have been found to behave more confidently during a negotiation task than people embodied in shorter avatars (57). Further, including larger groups will enable more profound investigations of the relationship between established psychiatric assessment measures and VR-assisted measures. Finally, coming research could benefit from the inclusion of participants on a spectrum from healthy controls to patients in clinical settings, and adopting a more transdiagnostic approach.
Limitations
This review has several limitations. First, only studies that were published in English were included, possibly limiting the evidence-base to draw conclusions upon. Second, this review concerns a relatively new technique, resulting in rather small sample sizes in the reviewed studies. A third limitation concerns the definition of adult samples; studies were included if either an age cut-off of 18 years and older was used (this was the case in the majority of the studies) or if the mean age was 18 years or older. Herewith also some adolescents were included in some studies which is a limitation. Also, a great variety of virtual environments and tasks were used in the included studies. Furthermore, studies were mixed in the use of a patient and control group, and not all studies provided results on relations between the VR-measures and traditional assessment measures. Additionally, some studies concerned a combination of VR-assisted assessment and treatment (40, 41), which made abstraction of the measures more difficult. However, in clinical practice, assessment will often be used to guide a therapeutic intervention. Therefore, one could also state that such trials combining both assessment and treatment closely approach the actual use in clinical settings. Finally, we did not include conference proceedings, which presents a limitation in such a new field as the current, with rapid developments.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
CG and MW designed the study. CG performed the literature search and wrote the first draft of the manuscript. CG and KS carried out the analysis of the results. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
Region Kronoberg (grant number 961523) and the Swedish Research Council for Health, Working Life and Welfare (grant number 2018-01409) have provided funding for this research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.828410/full#supplementary-material
References
1. Meyer GJ, Finn SE, Eyde LD, Kay GG, Moreland KL, Dies RR, et al. Psychological testing and psychological assessment: A review of evidence and issues. Am Psychol. (2001) 56:128–65. doi: 10.1037/0003-066X.56.2.128
2. Hermans K, Achterhof R, Myin-Germeys I, Kasanova Z, Kirtley O, Schneider M. Improving ecological validity in research on social cognition. In: Lewandowski KE, Moustafa AA, editors. Social Cognition in Psychosis. London: Elsevier (2019). pp. 249–68.
3. Castelvecchi D. Low-cost headsets boost virtual reality's lab appeal. Nature. (2016) 533:153–4. doi: 10.1038/533153a
4. Rus-Calafell M, Schneider S. Are we there yet?!—a literature review of recent digital technology advances for the treatment of early psychosis. mHealth. (2020) 6:3–3. doi: 10.21037/mhealth.2019.09.14
5. Slater M, Wilbur S. A Framework for Immersive Virtual Environments (FIVE): speculations on the role of presence in virtual environments. Presence Teleoper Virtual Environ. (1997) 6:603–16. doi: 10.1162/pres.1997.6.6.603
6. Martens MA, Antley A, Freeman D, Slater M, Harrison PJ, Tunbridge EM. It feels real: physiological responses to a stressful virtual reality environment and its impact on working memory. J Psychopharmacol. (2019) 33:1264–73. doi: 10.1177/0269881119860156
7. Veling W, Moritz S, van der Gaag M. Brave new worlds - review and update on virtual reality assessment and treatment in psychosis. Schizophr Bull. (2014) 40:1194–7. doi: 10.1093/schbul/sbu125
8. Skarbez R, Brooks FP, Whitton MC. A survey of presence and related concepts. ACM Comput Surv. (2017) 50:1–39. doi: 10.1145/3134301
9. Slater M. Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philos Trans R Soc B Biol Sci. (2009) 364:3549–57. doi: 10.1098/rstb.2009.0138
10. Freeman D, Reeve S, Robinson A, Ehlers A, Clark D, Spanlang B, et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. (2017) 47:2393–400. doi: 10.1017/S003329171700040X
11. Riva G. Virtual reality as assessment tool in psychology. Stud Health Technol Inform. (1997) 44:71–9.
12. van Bennekom MJ, de Koning PP, Denys D. Virtual reality objectifies the diagnosis of psychiatric disorders: a literature review. Front Psychiatry. (2017) 8:1–7. doi: 10.3389/fpsyt.2017.00163
13. Veling W, Brinkman W-P, Dorrestijn E, van der Gaag M. Virtual reality experiments linking social environment and psychosis: a pilot study. Cyberpsychol Behav Soc Netw. (2014) 17:191–5. doi: 10.1089/cyber.2012.0497
14. Fornells-Ambrojo M, Barker C, Swapp D, Slater M, Antley A, Freeman D. Virtual reality and persecutory delusions: safety and feasibility. Schizophr Res. (2008) 104:228–36. doi: 10.1016/j.schres.2008.05.013
15. Rus-Calafell M, Garety P, Sason E, Craig TJKK, Valmaggia LR. Virtual reality in the assessment and treatment of psychosis: a systematic review of its utility, acceptability and effectiveness. Psychol Med. (2017) 48:362–91. doi: 10.1017/S0033291717001945
16. Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. (2004) 1:176–84. doi: 10.1111/j.1524-475X.2004.04006.x
17. Ridout SJ, Spofford CM, van't Wout-Frank M, Philip NS, Unger WS, Carpenter LL, et al. Heart rate variability responses to a standardized virtual reality exposure in veterans with PTSD. Curr Treat Options Psychiatry. (2017) 4:271–80. doi: 10.1007/s40501-017-0118-9
18. Geraets CNW, van Beilen M, Pot-Kolder R, Counotte J, van der Gaag M, Veling W. Social environments and interpersonal distance regulation in psychosis: a virtual reality study. Schizophr Res. (2018) 192:96–101. doi: 10.1016/j.schres.2017.04.034
19. Camacho-Conde JA, Climent G, Antonio Camacho-Conde J, Climent G. Attentional profile of adolescents with ADHD in virtual-reality dual execution tasks: a pilot study. Appl Neuropsychol Child. (2020) 11:81–90. doi: 10.1080/21622965.2020.1760103
20. Fromberger P, Meyer S, Jordan K, Müller JL. Behavioral monitoring of sexual offenders against children in virtual risk situations: a feasibility study. Front Psychol. (2018) 9:224. doi: 10.3389/fpsyg.2018.00224
21. van 't Wout M, Spofford CM, Unger WS, Sevin EB, Shea MT. Skin conductance reactivity to standardized virtual reality combat scenes in veterans with PTSD. Appl Psychophysiol Biofeedback. (2017) 42:209–21. doi: 10.1007/s10484-017-9366-0
22. Malta LS, Giosan C, Szkodny LE, Altemus MM, Rizzo AA, Silbersweig DA, et al. Development of a virtual reality laboratory stressor. Virtual Real. (2021) 25:293–302. doi: 10.1007/s10055-020-00455-5
23. Provenzano L, Porciello G, Ciccarone S, Lenggenhager B, Tieri G, Marucci M, et al. Characterizing body image distortion and bodily self-plasticity in anorexia nervosa via visuo-tactile stimulation in virtual reality. J Clin Med. (2019) 9:98. doi: 10.3390/jcm9010098
24. Porras-Garcia B, Ferrer-Garcia M, Serrano-Troncoso E, Carulla-Roig M, Soto-Usera P, Miquel-Nabau H, et al. Validity of virtual reality body exposure to elicit fear of gaining weight, body anxiety and body-related attentional bias in patients with anorexia nervosa. J Clin Med. (2020) 9:3210. doi: 10.3390/jcm9103210
25. Summers BJ, Schwartzberg AC, Wilhelm S. A virtual reality study of cognitive biases in body dysmorphic disorder. J Abnorm Psychol. (2021) 130:26–33. doi: 10.1037/abn0000563
26. Shaikh M, Ellett L, Dutt A, Day F, Laing J, Kroll J, et al. Perceived ethnic discrimination and persecutory paranoia in individuals at ultra-high risk for psychosis. Psychiatry Res. (2016) 241:309–14. doi: 10.1016/j.psychres.2016.05.006
27. Veling W, Pot-Kolder R, Counotte J, van Os J, van der Gaag M. Environmental social stress, paranoia and psychosis liability: a virtual reality study. Schizophr Bull. (2016) 42:1363–71. doi: 10.1093/schbul/sbw031
28. Hesse K, Schroeder PA, Scheeff J, Klingberg S, Plewnia C. Experimental variation of social stress in virtual reality - feasibility and first results in patients with psychotic disorders. J Behav Ther Exp Psychiatry. (2017) 56:129–36. doi: 10.1016/j.jbtep.2016.11.006
29. Dietrichkeit M, Grzella K, Nagel M, Moritz S. Using virtual reality to explore differences in memory biases and cognitive insight in people with psychosis and healthy controls. Psychiatry Res. (2020) 285:112787. doi: 10.1016/j.psychres.2020.112787
30. Diemer J, Lohkamp N, Mühlberger A, Zwanzger P. Fear and physiological arousal during a virtual height challenge—effects in patients with acrophobia and healthy controls. J Anxiety Disord. (2016) 37:30–9. doi: 10.1016/j.janxdis.2015.10.007
31. Breuninger C, Sláma DM, Krämer M, Schmitz J, Tuschen-Caffier B. Psychophysiological reactivity, interoception and emotion regulation in patients with agoraphobia during virtual reality anxiety induction. Cogn Ther Res. (2017) 41:193–205. doi: 10.1007/s10608-016-9814-9
32. Kishimoto T, Ding X. The influences of virtual social feedback on social anxiety disorders. Behav Cogn Psychother. (2019) 47:726–35. doi: 10.1017/S1352465819000377
33. Felnhofer A, Hlavacs H, Beutl L, Kryspin-Exner I, Kothgassner OD. Physical presence, social presence, and anxiety in participants with social anxiety disorder during virtual cue exposure. Cyberpsychol Behav Soc Netw. (2019) 22:46–50. doi: 10.1089/cyber.2018.0221
34. Kim H, Shin JE, Hong Y-J, Shin Y-BYS, Shin Y-BYS, Han K, et al. Aversive eye gaze during a speech in virtual environment in patients with social anxiety disorder. Aust N Z J Psychiatry. (2018) 52:279–85. doi: 10.1177/0004867417714335
35. Guitard T, Bouchard SS, Bélanger C, Berthiaume M, Belanger C, Berthiaume M, et al. Exposure to a standardized catastrophic scenario in virtual reality or a personalized scenario in imagination for generalized anxiety disorder. J Clin Med. (2019) 8:309. doi: 10.3390/jcm8030309
36. Holmberg TT, Eriksen TL, Petersen R, Frederiksen NNN, Damgaard-Sorensen U, Lichtenstein MB, et al. Social anxiety can be triggered by 360-degree videos in virtual reality: a pilot study exploring fear of shopping. Cyberpsychol Behav Soc Netw. (2020) 23:495–9. doi: 10.1089/cyber.2019.0295
37. Wang Y-G, Shen Z-H, Wu X-C. Detection of patients with methamphetamine dependence with cue-elicited heart rate variability in a virtual social environment. Psychiatry Res. (2018) 270:382–8. doi: 10.1016/j.psychres.2018.10.009
38. Ding X, Li Y, Li D, Li L, Liu X. Using machine-learning approach to distinguish patients with methamphetamine dependence from healthy subjects in a virtual reality environment. Brain Behav. (2020) 10:e01814. doi: 10.1002/brb3.1814
39. Ghita A, Hernandez-Serrano O, Fernandez-Ruiz Y, Monras M, Ortega L, Mondon S, et al. Cue-elicited anxiety and alcohol craving as indicators of the validity of ALCO-VR software: a virtual reality study. J Clin Med. (2019) 8:1153. doi: 10.3390/jcm8081153
40. Bouchard S, Robillard G, Giroux I, Jacques C, Loranger C, St-Pierre M, et al. Using virtual reality in the treatment of gambling disorder: the development of a new tool for cognitive behavior therapy. Front Psychiatry. (2017) 8:27. doi: 10.3389/fpsyt.2017.00027
41. Chrétien M, Giroux I, Goulet A, Jacques C, Bouchard SS, Chretien M, et al. Using virtual reality to elicit dysfunctional thoughts in individuals with gambling disorder. J Gambl Issues. (2018) 2018:169–89. doi: 10.4309/jgi.2018.38.9
42. Shin Y-B, Kim J-J, Kim M-K, Kyeong S, Jung YH, Eom H, et al. Development of an effective virtual environment in eliciting craving in adolescents and young adults with internet gaming disorder. PLoS ONE. (2018) 13:e0195677. doi: 10.1371/journal.pone.0195677
43. Lee N, Kim J-J, Shin Y-B, Eom H, Kim M-K, Kyeong S, et al. Choice of leisure activities by adolescents and adults with internet gaming disorder: development and feasibility study of a virtual reality program. JMIR Serious Games. (2020) 8:e18473. doi: 10.2196/18473
44. Lorenzo G, Lledó A, Arráez-Vera G, Lorenzo-Lledó A. The application of immersive virtual reality for students with ASD: a review between 1990–2017. Educ Inf Technol. (2019) 24:127–51. doi: 10.1007/s10639-018-9766-7
45. Duffield TC, Parsons TD, Landry A, Karam S, Otero T, Mastel S, et al. Virtual environments as an assessment modality with pediatric ASD populations: a brief report. Child Neuropsychol. (2018) 24:1129–36. doi: 10.1080/09297049.2017.1375473
46. Renaud P, Chartier S, Rouleau JL, Proulx J, Goyette M, Trottier D, et al. Using immersive virtual reality and ecological psychology to probe into child molesters' phenomenology. J Sex Aggress. (2013) 19:102–20. doi: 10.1080/13552600.2011.617014
47. Sygel K, Wallinius M. Immersive virtual reality simulation in forensic psychiatry and adjacent clinical fields: a review of current assessment and treatment methods for practitioners. Front Psychiatry. (2021) 12:673089. doi: 10.3389/fpsyt.2021.673089
48. Webb AK, Vincent AL, Jin AB, Pollack MH. Physiological reactivity to nonideographic virtual reality stimuli in veterans with and without PTSD. Brain Behav. (2015) 5:1–9. doi: 10.1002/brb3.304
49. Bailey JO, Bailenson JN. When does virtual embodiment change our minds? Presence Teleoperators Virtual Environ. (2016) 25:222–33. doi: 10.1162/PRES_a_00263
50. Waltemate T, Gall D, Roth D, Botsch M, Latoschik ME. The impact of avatar personalization and immersion on virtual body ownership, presence, and emotional response. IEEE Trans Vis Comput Graph. (2018) 24:1643–52. doi: 10.1109/TVCG.2018.2794629
51. Freeman D, Pugh K, Green C, Valmaggia L, Dunn G, Garety P. A measure of state persecutory ideation for experimental studies. J Nerv Ment Dis. (2007) 195:781–4. doi: 10.1097/NMD.0b013e318145a0a9
52. Pot-Kolder R, Geraets CNW, Veling W, Staring ABP, Gijsman HJ, Delespaul PA, et al. Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: a single-blind randomised controlled trial. Lancet Psychiatry. (2018) 5:217–26. doi: 10.1016/S2215-0366(18)30053-1
53. Riches S, Bird L, Chan N, Garety P, Rus-Calafell M, Valmaggia L. Subjective experience of paranoid ideation in a virtual reality social environment: a mixed methods cross-sectional study. Clin Psychol Psychother. (2020) 27:337–45. doi: 10.1002/cpp.2431
54. Insel T, Cuthbert B, Garvey M, Heinssen R, Pine D, Quinn K, et al. Research Domain Criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry Online. (2010) 167:748–51. doi: 10.1176/appi.ajp.2010.09091379
55. Bittencourt J, Velasques B, Teixeira S, Basile LF, Salles JI, Nardi AE, et al. Saccadic eye movement applications for psychiatric disorders. Neuropsychiatr Dis Treat. (2013) 9:1393–409. doi: 10.2147/NDT.S45931
56. Del Valle Rubido M, McCracken JT, Hollander E, Shic F, Noeldeke J, Boak L, et al. In search of biomarkers for autism spectrum disorder. Autism Res. (2018) 11:1567–79. doi: 10.1002/aur.2026
Keywords: virtual reality, assessment, diagnostic, psychiatry, mental disorder
Citation: Geraets CNW, Wallinius M and Sygel K (2022) Use of Virtual Reality in Psychiatric Diagnostic Assessments: A Systematic Review. Front. Psychiatry 13:828410. doi: 10.3389/fpsyt.2022.828410
Received: 03 December 2021; Accepted: 03 February 2022;
Published: 28 February 2022.
Edited by:
Uffe Kock Wiil, University of Southern Denmark, DenmarkReviewed by:
Sebastian Oberdörfer, Julius Maximilian University of Würzburg, GermanyMariano Alcañiz, Universitat Politècnica de València, Spain
Copyright © 2022 Geraets, Wallinius and Sygel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chris N. W. Geraets, Yy5uLncuZ2VyYWV0c0B1bWNnLm5s